23 April 2025
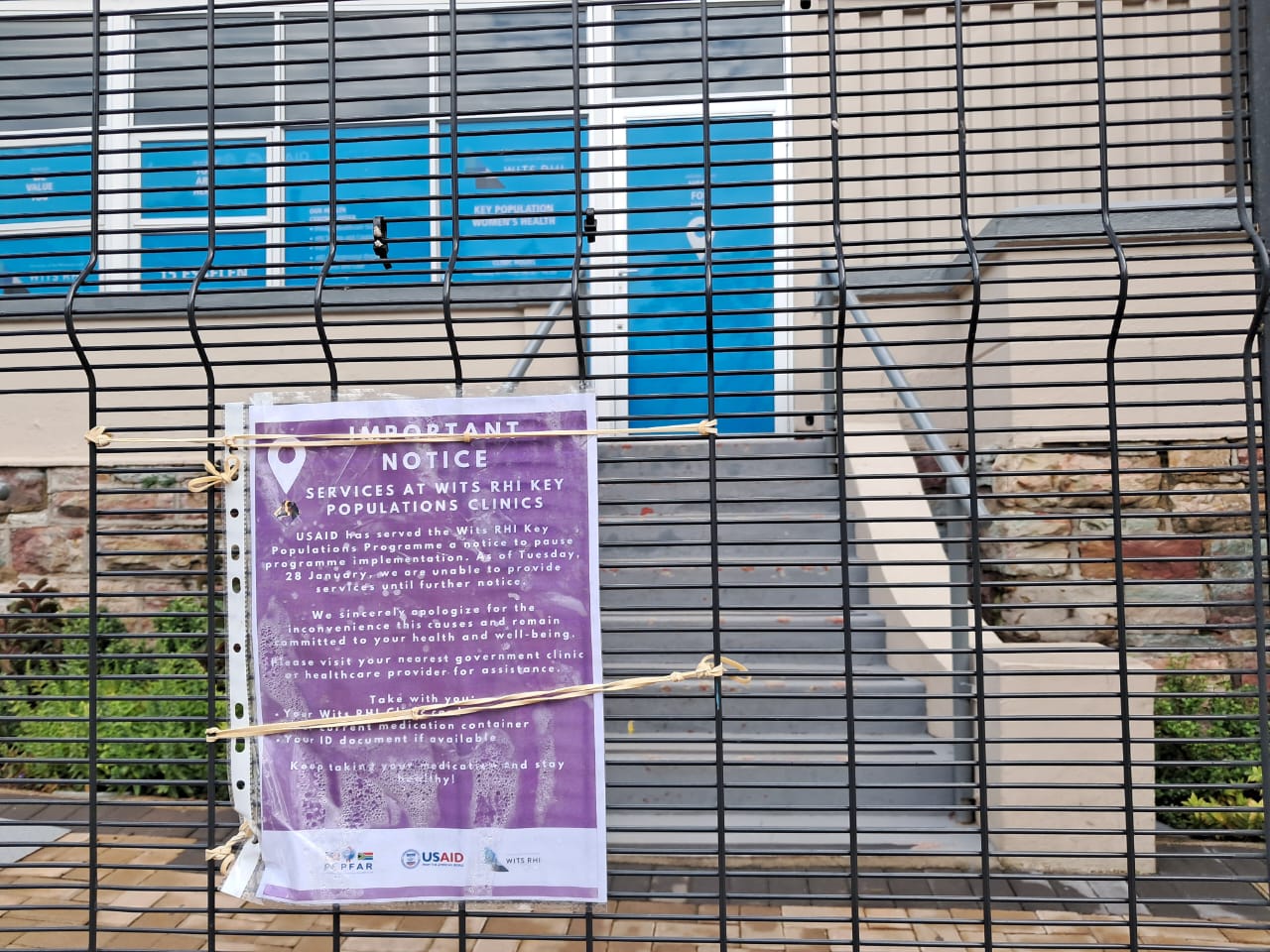
Sign outside a closed US-funded clinic in Johannesburg. Archive photo: Ihsaan Haffejee
We’re watching the largest HIV treatment programme in the world unravelling in real time. We don’t need perfection, but we do need a combination of urgency, action, and strategy to save it, argues Professor Francois Venter.
We are about to see a wave of new HIV infections, sickness, and death, with children born infected in record numbers. We will see our public hospitals further overwhelmed, and our hard-won victories against TB reversed.
It is all preventable.
Two decades ago, South Africa’s HIV crisis was defined by denialism and delay. Then President Thabo Mbeki and the late Health Minister Manto Tshabalala-Msimang presided over a period in which scientific consensus was rejected and the rollout of antiretroviral medicines was obstructed, and preventable deaths spiralled into the hundreds of thousands. Their names are now linked to one of the worst public health failures in modern history.
The consequences of today’s inaction will also be deadly.
Sadly, Minister of Health Aaron Motsoaledi and President Cyril Ramaphosa are charting their own tragic legacy. This time, it isn’t denialism; it’s ignoring the problem.
The US has abruptly suspended almost all foreign development assistance globally, including the President’s Emergency Plan for AIDS Relief (PEPFAR) and National Institutes of Health (NIH) research grants.
In South Africa, NGO-led clinics closed overnight, stockouts were reported of antiretrovirals (ARVs), and thousands of workers across HIV programmes lost their jobs. MatCH, an organisation which provides vital HIV services, entered business rescue. ANOVA, also a major service provider, retrenched 2,000 staff. TAC/Ritshidze, which monitors the HIV programme, retrenched 75% of its team. 230,000 doses of long-acting injectable medicines that prevent HIV transmission have not been released due to the funding freeze.
You notice a system was working well when it is suddenly removed. Many South Africans may realise HIV hasn’t been on their minds or in the media much for the last 15 years. That is because the HIV response in South Africa is one of the health department’s few delivery jewels.
South Africa’s HIV response has made monumental strides over the past two decades:
Central to that success was PEPFAR, which funded a critical part of the system that held much of the HIV response together, built around the health department’s functional primary care clinic system.
The PEPFAR programme was efficient. Targets for testing were set, and over 200 technical experts were funded by PEPFAR to support the national and provincial health departments.
This pressure pushing a sluggish health department was essential. The competition and accountability mechanisms created the urgency needed to keep the system responsive and moving forward.
While HIV programmes unravel and lives are lost, Ramaphosa and the Government of National Unity (GNU) are nowhere to be seen. Motsoaledi, once praised for his HIV leadership, offers no leadership, communication, or urgency.
The current crisis, triggered by the US government funding withdrawal has meant:
HIV testing programmes have all but collapsed. Clear evidence from the COVID epidemic shows that fewer tests means far fewer people start treatment. Services to trace people who’ve fallen out of care are now halted. Key populations have effectively been abandoned. Community monitoring systems have been turned off. HIV data systems are dark. ARV supply chains are faltering. Programmes have been gutted that were advancing long-acting pre-exposure prophylaxis (PrEP), community outreach, and disease surveillance. Our world-class HIV and TB research cadre has been severely damaged.
And still, South African health and political leadership has not produced a plan, despite civil society repeatedly pleading for transparency. Help has been offered – by the private sector and donors, but spurned. The department has been slow to request funds from National Treasury. Instead the department has sent out a thin emergency circular that appears not to have been implemented at any level.
Motsoaledi announced a grand plan to get an additional 1.1-million people on treatment by the end of the year, but with no operational plan, no reprioritisation, and no budget.
It is difficult not to feel despair. I have seen the recent data on HIV testing, the PrEP numbers, the infant diagnostic stats, and, most shockingly, the viral load suppression figures, and they all paint the picture of a rapidly decaying system. I am seeing the consequences in Johannesburg’s inner city where I work.
A study commissioned by the health department suggests there will be between 56,000 and 65,000 additional deaths, and 150,000 new infections in just three years from the US withdrawal. TB experts predict 580,000 fewer people screened, and 35,000 fewer people on TB treatment in 2025. The World Health Organisation (WHO) estimates that health damage within Africa from the current funding cut is already, in just three months, the equivalent of 75% of COVID’s peak damage.
Yet I was told at a meeting of my senior university leadership to discuss the massive funding and job cuts, that the President, who appeared weekly on television during COVID, was “too busy with the G20” meeting to meet them. Civil society’s leading organisations confirmed to me last weekend that the President and Ministers have not responded to formal letters asking for a plan, despite emails pleading with them to do so, beyond acknowledgements of receipt. Motsoaledi has had one meeting with the NGOs, and only with selected partners.
The loss of hard-working NGO jobs was not met with concern, outrage, or even a word of thanks by the health department, but with a hostile press statement.
We are not where we were in 2004, at the height of Mbeki denialism, and it is good to remind ourselves of the many strengths of the HIV response and public health within our country.
We should have little patience for further delay and silence from our government. We cannot have a health department with no plan and, critically, no communication as to what is being done. Get the experts into the room, and get a plan together – with actual priorities, funding, targets, and partners. We don’t need perfection, but we do need urgency.
The health system that is delivering HIV care is unravelling now. A combination of action, strategy, and urgency can save us.
It will be hard. But the cost of doing nothing is millions of lives and a shattered legacy.